
Emotional Dysregulation is currently a hot topic in the ADHD community, in part due to ADDitude Magazines promoting the concept of Rejection Sensitivity Dysphoria (RSD) as a novel symptom of ADHD. It is not. Here’s why, and how this new concept may be counterproductive to reducing the misdiagnosis of ADHD as Borderline Personality Disorder (BPD), which today is a significant risk-factor, especially for women who are adult late-diagnosed with ADHD/BPD.
However, as we discuss below, evidence-based treatments are entirely different for the two disorders, suggesting that the underlying cause of the disrupted emotional circuits may differ in ADHD and BPD, potentially explaining differences in response to different treatments.
(Moukhtarian et al., 2018)
In this article I will compare and contrast Emotional Dysregulation in ADHD vs. BPD so that you as a licensed mental health professional will be better equipped to provide the correct diagnosis, and thereby the correct treatment plan, for each af these disorders.
In our ADDspeaker community on Facebook, where more than 500 adults are participating in science-based, factual, and reciprocal emotional, and social support, I have discovered a trend, and that that is that an unrealistic percentage of the (female) members, who have been late-diagnosed with ADHD, either previously as their primary or currently as a comorbid disorder, have been diagnosed with Borderline Personality Disorder (BPD).
As one of our goals in our community, is to encourage people to gain personal insights, based on scientific evidence, in order to them to get the best (and correct) treatment for their symptoms, I’ve researched how this discrepancy is likely rooted in overlapping symptomatology between ADHD and BPD due to their shared symptoms of Emotional Dysregulation (also referred to as Rejection Sensitivity Dysphoria by ADDitude Magazine and Dr. Dodson).
As I have discovered this dangerous trend of misdiagnosis of late-diagnosed women with Borderline Personality Disorder (BPD), where their primary diagnosis is actually ADHD, this poses a serious treatment problem, as BPD is a psychologically rooted disorder, whereas ADHD is a neuro-physiologically rooted disorder.
By misdiagnosing ADHD as BPD, these women spends years in ineffective, psychosocial treatment, when they should really have been pharmacologically treated for their (undiagnosed) ADHD instead.
As we know, undiagnosed and unmedicated ADHD causes the Estimated Life Expectancy to be reduced by 12,7 years, this is not a trivial matter! (Barkley et al., 2018).
In this article, I explain what the differences between ADHD and BPD are, and how you as a mental health service provider, can learn to spot the differences.
Even the earliest known definition of ADHD (1798) included affective instability as a core symptom, and in modern times, emotional instability was in the DSM up until […] DSM-II and progressing to the present, emotional dysregulation has been excluded from the clinical conceptualization of the disorder and the diagnostic criteria and relegated to an associated problem or the result of comorbid disorders […] (Barkley et al., 2015).
Emotional Dysregulation has become the talk of the town, but what is it, and why should we with ADHD even care about it?
Well, it’s a pretty essential part of our symptomatology, so we’ve better get a handle on it.
Here’s a few random quotes from Google:
“Emotional dysregulation (ED) is a term used in the mental health community to refer to an emotional response that is poorly modulated, and does not fall within the conventionally accepted range of emotive response.”
“Emotional dysregulation refers to the inability of a person to control or regulate their emotional responses to provocative stimuli. It can also be termed “emotional hyperreactivity.”
“Emotional dysregulation is characterized by difficulty in the regulation of emotional responses and behavior.”
“Emotional dysregulation (ED), also called ‘emotional hyperactivity’, means that you are more emotionally responsive than an average person. Your emotions will be triggered more quickly, and will tend to be on a bigger scale. You also have more difficulty controlling your emotions than others do. Your might often feel taken over and lost in your emotional states.”
As you can see, everyone is talking about Emotional Dysregulation, but few agree on what it actually is, right? The above quotes are littered with subjective definitions that are created to fit subjective agendas.
So I thought that I’d might have to ‘go down the rabbit hole’ and see if I could provide an ADHD-friendly definition, since ED is becoming more and more – reintroduced – as a core symptom of ADHD.
As this is a very complex topic to compare and contrast, with minute details that shows the nuanced differences, I have decided to rely heavily on citations for this part of my article, since I do not wish to add to the confusion by quoting misperceived, subjective interpretations of Emotional Dysregulation in ADHD vs. BPD.
Following this scientific run-through, I will return to my perspectival conclusions as so as to sum-up the key points, and thereby help you, as the person with ADHD, BPD (or both), or the licensed mental health professional performing the diagnosing.
ED is a dimensional construct, referring to rapid and exaggerated changes in emotional states such as heightened irritability or hot temper (Moukhtarian et al., 2018).
Comparing ED in ADHD and BPD shows why this often leads to a misdiagnosis of BPD, where the primary diagnosis should have been … ADHD.
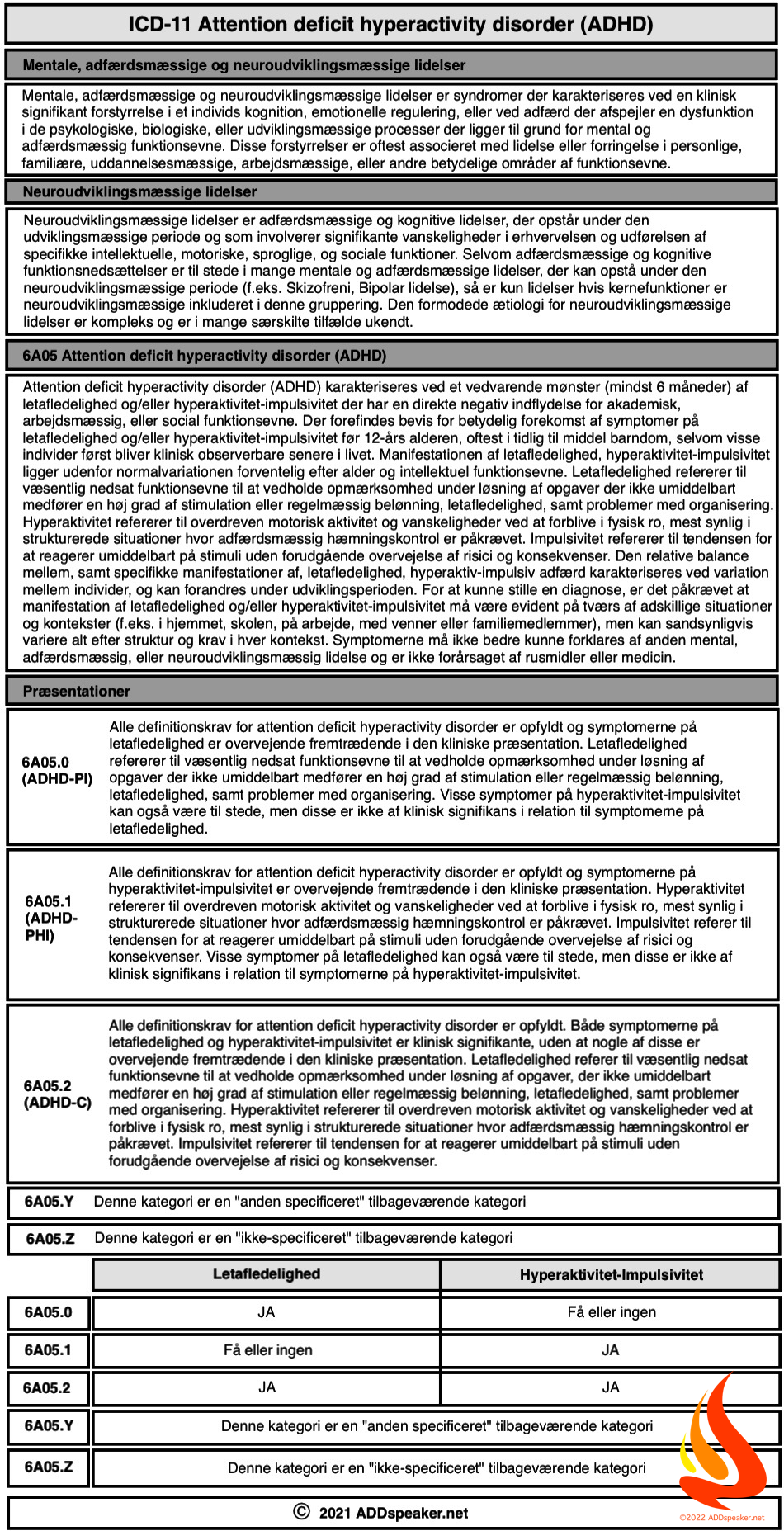
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM–5), the diagnosis of ADHD requires six out of nine ADHD symptoms of either inattention or hyperactivity/impulsivity in childhood, and five out of nine in adults (Table 1).
Additional criteria include childhood age of onset defined as several ADHD symptoms present before the age of 12 years, pervasiveness defined as symptoms present in two or more settings, and impairment defined as- interference with or reduced quality of social, academic or occupational functioning (Moukhtarian et al., 2018).
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder emerging in childhood or early adolescence, characterised by a pervasive pattern of developmentally inappropriate levels of inattention and/or hyperactivity-impulsivity that lead to clinically significant functional and psychosocial impairments (Moukhtarian et al., 2018).
The disorder affects around 5% of children (Moukhtarian et al., 2018).
Longitudinal follow-up studies of children with ADHD show that symptoms of ADHD commonly persist into adulthood, with around two-thirds of cases meeting either full or sub-threshold criteria in adulthood (Moukhtarian et al., 2018).
The prevalence of adult ADHD in epidemiological surveys is estimated at around 2.5–4% (Moukhtarian et al., 2018).
Although ADHD is recognised as a predominantly male disorder in childhood (clinic-referred children are more likely to be male), in adult samples the gender difference is less pronounced (Moukhtarian et al., 2018).
Apart from the main symptoms used to classify ADHD, ED is considered to be an associated feature supporting the diagnosis of ADHD (Moukhtarian et al., 2018).
In ADHD, ED is characterised by problems with temper control (feelings of irritability and frequent outburst of short duration), emotional over-reactivity (diminished ability to handle typical life stresses, resulting in frequent feelings of being hassled and overwhelmed), and mood lability (short and unpredictable shifts from normal mood to depression or mild excitement) (Moukhtarian et al., 2018).
ED has also been found to be an independent predictor of impairment in ADHD, after controlling for the confounding effects of core ADHD symptoms (inattention and hyperactivity/impulsivity) on impairment (Moukhtarian et al., 2018).
BPD is a complex and severe mental health disorder, with typical symptom onset during adolescence and presence of behavioural precursors in childhood, persisting into adulthood (Moukhtarian et al., 2018).
BPD is characterised by a pervasive pattern of unstable interpersonal relationships, pronounced impulsive and self-damaging behaviour, unstable identity, and difficulties with ED, which substantially impact in an enduring way on quality of life
and psychosocial functioning (Moukhtarian et al., 2018).
The DSM-5 diagnosis of BPD requires the pervasive presence of a minimum of five out of nine symptoms (Table 2) (Moukhtarian et al., 2018).
In the general population, BPD has a prevalence of around 6% and within populations of adult psychiatric inpatients, prevalence is around 20% (Moukhtarian et al., 2018).
Most epidemiological surveys report no gender differences of BPD,
yet studies of clinical populations typically report higher prevalence figures in women than in men. The different sex ratios in clinical and population samples may be explained by both assessment and sampling biases (Moukhtarian et al., 2018).
Like ADHD, individuals with BPD commonly present with comorbid mental health disorders. In particular, around 90% of BPD cases are reported to have co-occurring mood disorders including depression and dysthymia, along with a high prevalence of substance use disorders in the range of 15% to 57% (Moukhtarian et al., 2018).
Psychiatric comorbidity is commonly found across all
mental health disorders and is defined as the presence
of two or more disorders in the same individual at a given
time (Moukhtarian et al., 2018).
In principle, each of the disorders should make a
unique contribution to the clinical presentation of the in-
dividual (Moukhtarian et al., 2018).
However, estimates of comorbidity prevalence may be inflated if there is marked overlap in the symptom criteria of two disorders, leading to poor diagnostic delineation i.e. artefactual co-morbidity (Moukhtarian et al., 2018).
Furthermore, it remains unclear to what extent psychiatric
diagnoses reflect entirely distinct disorders, rather than
overlapping syndromes (Moukhtarian et al., 2018).
This is a particular problem for psychiatry since there are, as yet, no validated biomarkers or other objective markers with sufficient sensitivity or specificity to be used in clinical practice to distinguish aetiologically distinct mental health conditions (Moukhtarian et al., 2018).
Regarding ADHD and BPD, while the specific symptoms used to classify the two disorders are different, many clinical characteristics are shared, including ED, impulsive risk-taking behaviour, and unstable interpersonal relationships (Moukhtarian et al., 2018).
A high prevalence of co-occurring ADHD and BPD is consistently reported in the literature (Moukhtarian et al., 2018).
In a large in- and outpatient cohort of 372 adults with ADHD referred for ADHD assessment and treatment at a tertiary referral
centre, 27.2% also met criteria for BPD assessed by the structured clinical Interview for DSM-IV II (SCID II) (Moukhtarian et al., 2018).
Similarly, in another sample of 335 adults referred by family physicians, community health clinics or self-referred, BPD, assessed by the SCID-II, was reportedly present in 10% of participants with DSM-IV inattentive subtype ADHD (six or more symptoms in inattention) and 24% of participants with combined subtype ADHD (six or more symptoms of both inattention and hyperactivity/impulsiviity) (Moukhtarian et al., 2018).
Likewise, in a sample of 181 adult patients diagnosed with BPD by general practitioners and referred for treatment, 38.1% had comorbid ADHD, with 22.7% meeting the combined type criteria (Moukhtarian et al., 2018).
In a sample of 118 adult women from out-patient clinics seeking treatment for BPD, a high co-occurrence rate was reported: 41.5% met criteria for childhood ADHD (assessed retrospectively), and 16.1% met current criteria for the DSM-IV combined subtype, as well as meeting ADHD criteria as children (Moukhtarian et al., 2018).
In a sample of adolescents (n = 107) with emerging BPD drawn from a European research project investigating the phenomenology of BPD in adolescence, the prevalence of ADHD was 11%, an estimate that was not attenuated even when excluding symptoms of impulsivity accounting for possible symptom overlap (Moukhtarian et al., 2018).
This rate was close to the 16% rate found by Philipsen and colleagues, where current ADHD symptoms was assessed by self-report measures, as opposed to clinician-based interviews. Moreover, the samples significantly differed in regard to participants’ age (Moukhtarian et al., 2018).
Regarding population samples, results from the National Epidemiologic Survey on Alcohol and Related Conditions of more than n = 34,000 adults, found that lifetime comorbidity with BPD in the ADHD population was 33.7% compared with a lower prevalence of BPD of only 5.2% in the general population (Moukhtarian et al., 2018).
There is considerable overlap in the symptoms of BPD and the associated features of ADHD (Table 3).
Considering the onset and developmental trajectory, both disorders can be considered ‘developmental’ in the sense that they both emerge during childhood or adolescence and reflect enduring trait-like (non-episodic) symptoms and behaviours (Moukhtarian et al., 2018).
The shared general features of trait-like symptoms that characterise both ADHD and BPD; means that differentiating between these diagnoses cannot easily be established by considering age of onset and course of symptoms (Moukhtarian et al., 2018).
This means that to a large extent, differential diagnosis is based on the specific symptoms and behaviours used to define the two disorders (Moukhtarian et al., 2018).
The most noticeable overlap among the core symptoms used to classify both conditions is impulsivity (Moukhtarian et al., 2018).
Nevertheless, there are important qualitative differences in the manifestation of impulsivity used in the classification of ADHD and BPD (Moukhtarian et al., 2018).
In ADHD, impulsivity refers to difficulty waiting or taking turn, blurting out during conversations (e.g. interrupting or talking over people), and intruding on others (e.g. butting into conversations or activities, taking over what others are doing) (Moukhtarian et al., 2018).
These impulsive symptoms are not always severe in adults with ADHD, but when severe can lead to impairment in social functioning and self-damaging or risk-taking behaviour (Moukhtarian et al., 2018).
The consequences of severe impulsivity in ADHD include reckless driving, promiscuity, interpersonal relationship problems and aggressive behaviour (Moukhtarian et al., 2018).
In BPD, impulsivity is defined by self-damaging behaviour, such as reckless driving, shoplifting, spending, binge eating, substance abuse and promiscuity (Moukhtarian et al., 2018).
People with either of these disorders may therefore display impulsive risk-taking behaviour, but from a diagnostic point of view they are core symptom of the BPD diagnosis, but only an associated feature of ADHD (Moukhtarian et al., 2018).
The other key area of symptom overlap is ED. This reflects a core symptom domain in the diagnostic classification of BPD, whereas in ADHD it is recognised as an associated clinical feature that supports the diagnosis (Moukhtarian et al., 2018).
Nevertheless, ED is commonly seen to accompany ADHD, even in non-comorbid cases, and is an independent source of psychosocial impairment (Moukhtarian et al., 2018).
This draws strong comparisons with ED in BPD, particularly when the ED that accompanies ADHD is severe (Moukhtarian et al., 2018).
At a descriptive level, the emotional symptoms of ADHD
were well captured by Wender, Reimherr and colleagues
in the earlier Wender-Utah criteria for ADHD, and show
substantial overlap with the ED symptoms in the DSM-5
BPD criteria (Moukhtarian et al., 2018).
ED is a dimensional construct, referring to rapid and exaggerated changes in emotional states such as heightened irritability or hot temper (Moukhtarian et al., 2018).
A review by Asherson and colleagues reported that ED is present in
72–90% of adults with ADHD, and independently of other symptoms of ADHD predicts impairments in social, educational and occupational domains (Moukhtarian et al., 2018).
In contrast, ED is one of the core symptom domains of individuals with BPD, who nearly always suffer from severe persistent affective instability, inner tension and difficulty controlling emotions such as anger (Moukhtarian et al., 2018).
Despite similarities, it has been suggested that patients with BPD have higher frequency and intensity of affective instability and
aggressive impulsive reactions, compared to adults with
ADHD (Moukhtarian et al., 2018).
Others describe ADHD patients as being high novelty seekers, who regulate their emotions through extreme external stimulation (e.g. sexual activity, aggressive behaviour), as opposed to those with BPD who tend to engage in self-mutilating behaviour to alleviate
negative affect and inner tension (Moukhtarian et al., 2018).
However, self- harming behaviour and suicidality in ADHD has been highlighted in recent literature (Moukhtarian et al., 2018).
Yet, phenomenologically, ED is a complex construct, with shared characteristics in both ADHD and BPD, particularly pertaining to feelings of heightened anger and difficulty controlling anger (criterion eight in BPD) (Moukhtarian et al., 2018).
Others suggest that emotional instability reflects a similar cyclothymic temperament pattern in both disorders (Moukhtarian et al., 2018).
Overall, it remains unclear whether the type of ED seen in ADHD really is qualitatively similar or different from that seen in BPD (Moukhtarian et al., 2018).
The overlap in symptoms of emotional dysregulation in ADHD and BPD raises the question of a common neurobiological substrate for ED in the two conditions (Moukhtarian et al., 2018).
In ADHD two competing hypotheses have been proposed for ED (Moukhtarian et al., 2018).
First, the ‘dyscontrol hypothesis’ proposes that ED is driven by the same cognitive and neural processes that drive ADHD; for example, deficits in top-down executive control, or bottom up state regulation factors [64]. In this model, ED reflects an alternative expression of the same underlying neurocognitive deficits
that lead to ADHD symptoms (Moukhtarian et al., 2018).
The alternative ‘affectivity hypothesis’ states that ED reflects deficits in neural processes related directly to emotional regulation, separate from those that lead to ADHD symptoms (Moukhtarian et al., 2018).
To date the accumulating evidence is pointing to the affectivity
hypothesis. Two key publications support this conclusion (Moukhtarian et al., 2018).
First, an investigation of cognitive performance deficits in ADHD (including inhibition, working memory, impulsive responding, slow and variable reaction times) found these were associated with ADHD symptoms independently from ED (Moukhtarian et al., 2018).
This suggests that different processes would explain the presence of ED in ADHD. Subsequently, a resting state functional Magnetic Resonance Imaging (fMRI) study in children with ADHD, found that ED, independently from ADHD, were associated with increased positive intrinsic functional connectivity (iFC) between bilateral amygdala and medial prefrontal regions, and reduced iFC between
amygdala and bilateral insula/superior temporal gyrus (Moukhtarian et al., 2018).
These findings suggested that ED is linked to disruptions in emotional control networks, which was not linked directly to ADHD (Moukhtarian et al., 2018).
Regarding BPD there are overlapping findings implicating the central role of emotional control networks (Moukhtarian et al., 2018).
A critical review of fMRI studies conclude that emotional sensitivity, including emotional hypersensitivity and intense emotional reactions, was associated with increased amygdala activity and decreased activity with prefrontal cortical control regions (Moukhtarian et al., 2018).
In particular a consistent decrease in anterior cingulate activity and variable was identified, while the medial and dorsolateral prefrontal areas showed variable activity across studies. Overall, increased limbic and diminished pre-frontal cortical activity suggested an impaired fronto-limbic inhibitory network (Moukhtarian et al., 2018).
Resting-state fMRI, contrasting intrinsic functional connectivity before and after an emotion regulation task in patients with BPD, further supports disrupted regulation of emotional circuits (Moukhtarian et al., 2018).
Emotional hypersensitivity in BPD was associated with increased intrinsic connectivity between the amygdala and bilateral insula together with dorsal anterior cingulate cortex, while their impaired control over emotional reactions was associated with diminished intrinsic connectivity between the central executive fronto-parietal regions and salience network (Moukhtarian et al., 2018).
Overall the pattern of findings in relation to emotion regulation was similar to that reported for ADHD by Hulvershorn and colleagues (Moukhtarian et al., 2018).
The overlap of these findings in relation to ED in the two disorders suggests that there may be a common substrate for ED in the two conditions, involving altered top down and bottom up regulation of amygdala function and neural circuits (Moukhtarian et al., 2018).
However, as we discuss below, evidence-based treatments are entirely different for the two disorders, suggesting that the underlying cause of the disrupted emotional circuits may differ in ADHD and BPD, potentially explaining differences in response to different treatments (Moukhtarian et al., 2018).
Nevertheless, these findings suggest that there could also be common forms of treatment in a least a subset of patients with a comparable neurobiological basis for ED (Moukhtarian et al., 2018).
As ADHD needs medicinal treatment as first-line, as opposed to BPD where group-based CBT is best-practice, many of these misdiagnosed women are receiving the wrong and ineffective psychosocial treatment, when they need a pharmacological treatment instead.
This creates real and life-long consequences for these women, as they may spend years trying to treat their Emotional Dysregulation symptoms using techniques designed for BPD, instead of the scientifically consensus of using pharmacological treatments.
This means that the consensus ‘best practice guidelines’ for treatment of BPD is psychosocial, group-based CBT, as opposed to ADHD where the neurochemical and pharmacological treatment is undeniably first-line and then psychosocial, individual/group-based CBT when the medication’s efficacy and tolerance, have been firmly established.
Treatment approaches to ADHD and BPD are widely divergent. According to evidence-based clinical guidelines, in BPD there is limited evidence that medications reduce borderline personality symptoms, including ED, and psychological treatments are the cornerstone of treatment (Moukhtarian et al., 2018).
In contrast, in ADHD there is good evidence for effects of medication on reducing ADHD symptoms and ED, and only limited evidence for effects of psychological treatments (Moukhtarian et al., 2018).
In contrast to treatment of ADHD, psychotherapy is regarded as first line treatment for people with BPD (Moukhtarian et al., 2018).
The most common therapies are:
(Moukhtarian et al., 2018)
DBT, the most intensively studied intervention for BPD, significantly reduces anger (Standardized Mean Difference (SMD) = − 0.83) and self-harm (SMD = − 0.54), and improves overall mental health functioning (SMD = 0.65) (Moukhtarian et al., 2018).
Not only is psychotherapy regarded as first line treatment for BPD, UK NICE guidelines stipulate that pharmacological treatments should not be used for managing BPD, nor for individual symptoms or behaviours associated with the disorder (Moukhtarian et al., 2018).
Currently, there is insufficient data on the treatment of co-occurring BPD and ADHD. With regard to drug treatment, there have been no RCTs of stimulants or atomoxetine in BPD alone or in co-occurring BPD-ADHD cases (Moukhtarian et al., 2018).
After reviewing the literature (see References for more studies, that I have consulted as well), and subsequently compared the scientific evidence with my personal knowledge from coaching more than 50 women with late-diagnosed ADHD (where I estimated that much as 1/3 was originally (potentially) misdiagnosed with BPD, I have created a treatment model for this group of women, in order for me to help them explain to their licensed mental health professional, why this person should reassess their initial BPD diagnosis, in light of the new scientific findings, so as to ensure that they where provide the correct diagnosis and thereby the correct treatment for their relevant disorder.
What we have learned, in the ADDspeaker community, during the past 2 years of intense scientific research and citizen scientific projects of our own, is that there is a alarming high rate of misdiagnosing (in Denmark at least, where we are based), and that the diagnosing mental health professionals are ill-equipped to understand the subtle nuances between ED in ADHD and ED in BPD, causing them to (unknowingly, not out of malaise) misdiagnose this particular group of women.
To further strengthen our community knowledge (and to verify the validity of our internal findings, which of course, by no means meet the standards of peer-reviewed, published literature) we have conducted extensive dialogue with world-leading scientists in the field of ADHD scientific research, as well as worked closely with experienced, top-ranking psychiatrists in the clinical practice in Denmark.
What this cooperation have provided (again indications of, not peer-reviewed scientific evidence for) is that when a person with a diagnosis of BPD, is reassessed under the ED criteria in ADHD, and subsequently treated with a pharmacological “Triad-treatment” of an antidepressant (low dosages) + non-stimulant (Guanfacine) (low dosages) + stimulant (Lisdexamfetamine) (recommended daily dosages), these women would experienced a significant reduction in the strength, duration, and intensity of the ED symptoms.
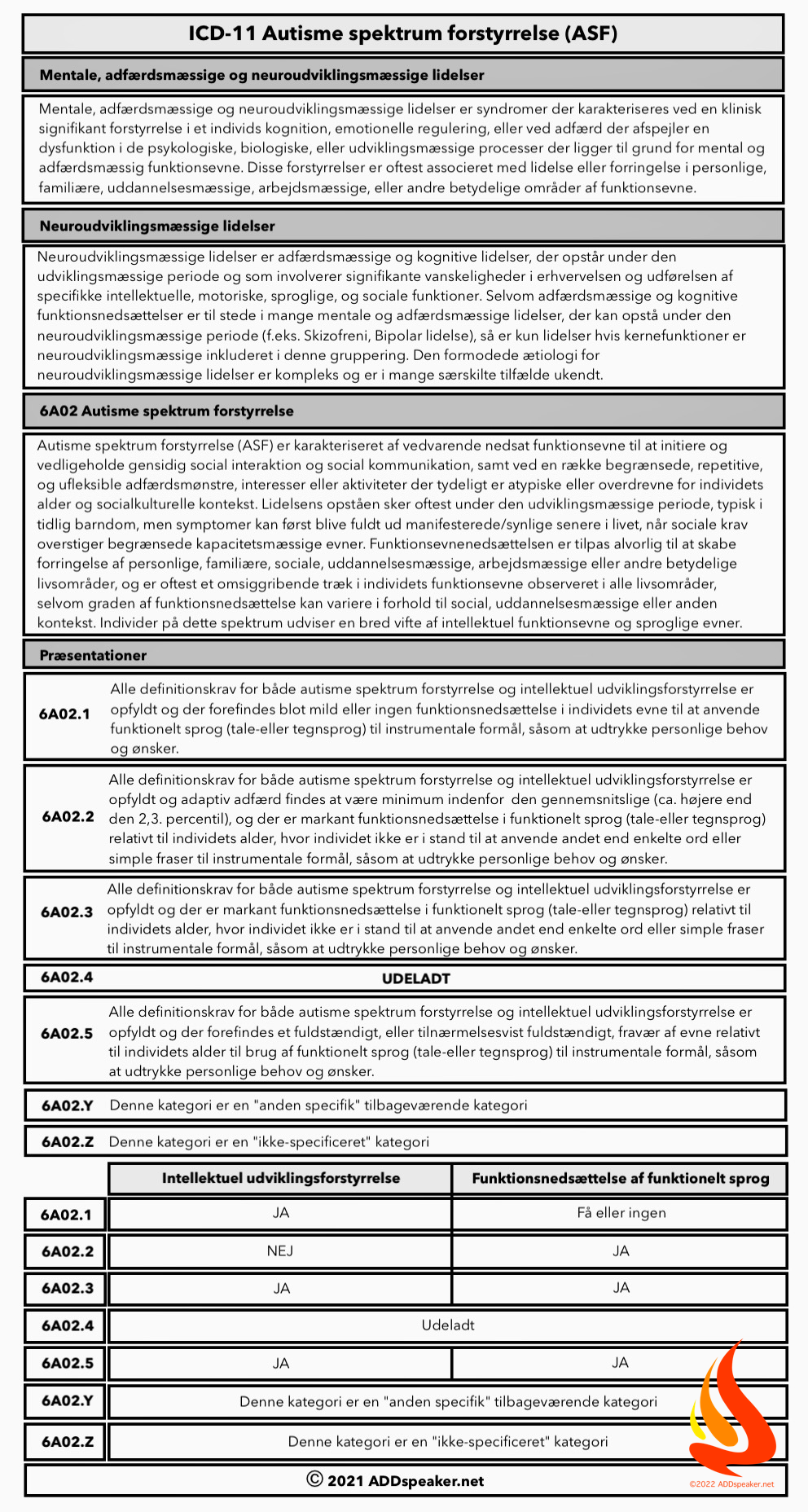
This created a foundation for introducing our internal ADDspeaker model for CBT, which is based on various well-known therapies like “5 Stages of Grief” (Kübler-Ross), “Logical Levels” (Robert Dilts), and furthermore cross-checking for comorbid Autism (since 50-70% of all persons with Autism have comorbid ADHD, and 25-30% of persons with ADHD have comorbid Autism) (Sokolova et al., 2017) using the Systemizer framework (Simon Baron-Cohen) and the Five-Factor Model (Goldberg).
By firstly routing out potential misnomers that could muddy the waters (in particular ‘Masking’ symptoms from Autism), we were able to show a significant and last-lasting (3 months and 6 month follow-ups) in their subjectively perceived Quality-of-Life, as well as their measurable severity of ADHD symptoms (ADHD-RS).
The most important result of this citizen scientist project, was the remarkable cross-over information sharing between our community, mental health professionals, the scientific community, and the personal, individual stories from the women within this project.
I’ve created a loving term for these women calling them “My Bat Shit Crazy Women”, and the now where this distinction as a kinda badge of honor, to show themselves, and each-other, that they are not alone in their emotional dysregulated day-to-day lives, and that what they are struggling with in terms of managing their plethora of symptoms, is not unique to them, but common to them all, and this have given them a major boost in their self-image, self-confidence, and self-love.
In conclusion, my hope for sharing this story of ours with you, is to give your the insight to embrace this knowledge that we’ve gather for you, in the hope that you also will be able to broaden your own clinical knowledge to include the – possibility – of your clients may as well be able to realize the same remarkable increase in their Quality-of-Life, as we so proudly have, within our Not-For-Profit, unaffiliated, peer-group online support network at ADDspeaker.
/ADDspeaker
Barkley R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychological bulletin, 121(1), 65–94. doi:10.1037/0033-2909.121.1.65
Barkley, R. A. (Ed.). (2015). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (4th ed.). New York, NY, US: Guilford Press.
Barrett L. F. (2017). The theory of constructed emotion: an active inference account of interoception and categorization. Social cognitive and affective neuroscience, 12(1), 1–23. doi:10.1093/scan/nsw154
Brookman-Frazee, L., Stadnick, N., Chlebowski, C., Baker-Ericzén, M., & Ganger, W. (2017). Characterizing psychiatric comorbidity in children with autism spectrum disorder receiving publicly funded mental health services. Autism, 136236131771265.doi:10.1177/1362361317712650
Jonkman, L. M., Markus, C. R., Franklin, M. S., & van Dalfsen, J. H. (2017). Mind wandering during attention performance: Effects of ADHD-inattention symptomatology, negative mood, ruminative response style and working memory capacity. PLOS ONE, 12(7), e0181213. doi:10.1371/journal.pone.0181213
Lenzi, F., Cortese, S., Harris, J., & Masi, G. (2018). Pharmacotherapy of emotional dysregulation in adults with ADHD: A systematic review and meta-analysis. Neuroscience and biobehavioral reviews, 84, 359–367. doi:10.1016/j.neubiorev.2017.08.010
Moukhtarian et al. Borderline Personality Disorder and Emotion Dysregulation (2018) 5:9, https://doi.org/10.1186/s40479-018-0086-8
Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E. (2014). Emotion dysregulation in attention deficit hyperactivity disorder. The American journal of psychiatry, 171(3), 276–293. doi: 10.1176/appi.ajp.2013.13070966
Sokolova, E., Oerlemans, A. M., Rommelse, N. N., Groot, P., Hartman, C. A., Glennon, J. C., … Buitelaar, J. K. (2017). A Causal and Mediation Analysis of the Comorbidity Between Attention Deficit Hyperactivity Disorder (ADHD) and Autism Spectrum Disorder (ASD). Journal of Autism and Developmental Disorders, 47(6), 1595–1604.doi:10.1007/s10803-017-3083-7
Sterling P. (2012). Allostasis: a model of predictive regulation. Physiology & behavior, 106(1), 5–15. doi:10.1016/j.physbeh.2011.06.004
This website uses cookies.



Tilføj din kommentar her - Feedback er altid velkomment!